How Denying Community Transmission Is Hampering India’s COVID-19 Response

Navi Mumbai: Even as Kerala confirmed there was community transmission in the state, the government of India has remained silent on it. The government, till date, maintains there is “no community transmission”, despite more than a million confirmed COVID-19 cases, the third highest in the world, behind only the United States and Brazil. This denial of what the experts are calling “the writing on the wall” is hurting the administration’s ability to build trust, communicate effectively and mobilise communities during the crisis, and hurting India’s handling of the pandemic.
Community transmission occurs when a positive patient has not been exposed to another known COVID-19 patient. This indicates that the infection is well-established in the community.
Quarantine and lockdown, which India is still focusing on, as a primary strategy is counterproductive, said experts. Instead, the focus should now be on community-driven behavioural changes, use of masks in public and a stronger message for hand washing, hygiene and social distancing, they said. Meanwhile, cities such as Delhi, Mumbai and Chennai, where the cases are no longer in mere clusters, ought to focus on getting only those with severe symptoms to hospitals while asking the mild and asymptomatic patients to stay at home.
Living in denial
India is definitely not in community transmission, insisted Balram Bhargava, director general of Indian Council of Medical Research (ICMR), during a press conference on June 11. “We have to continue our strategy of testing, tracing, tracking and quarantining and continue with the containment measures,” Bhargava said.
The government reiterated its stand on July 9, its last press conference on the pandemic. “A mere 49 districts account for 80% of our cases,” said Rajesh Bhushan, officer on special duty at the Ministry of Health and Family Welfare. India has had 1,118,043 COVID-19 cases as of 8 a.m. on July 20, behind only the United States and Brazil.
Kerala effectively implemented the test, isolate and contact trace strategy in February and March, after detecting its first COVID-19 case on January 30. But cases have surged once again in Kerala. Karnataka, which had been successful in containing cases, is also witnessing an unprecedented rise in COVID-19 cases and has imposed a new strict lockdown in Bengaluru from July 14 to 22.
While the Kerala government confirmed community transmission in some pockets, Karnataka has refused to attribute its latest spike to community transmission. Kerala was already looking for evidence of community transmission, said Jayaprakash Muliyil, an epidemiologist and former principal of Christian Medical College, Vellore. “Kerala would be the first state to declare it,” he had told IndiaSpend a few days before the state’s official announcement.
West Bengal too followed soon after and confirmed community transmission in some areas.
Meanwhile, neither the ICMR nor the central government has issued any official statement or held a press conference since Kerala’s announcement.
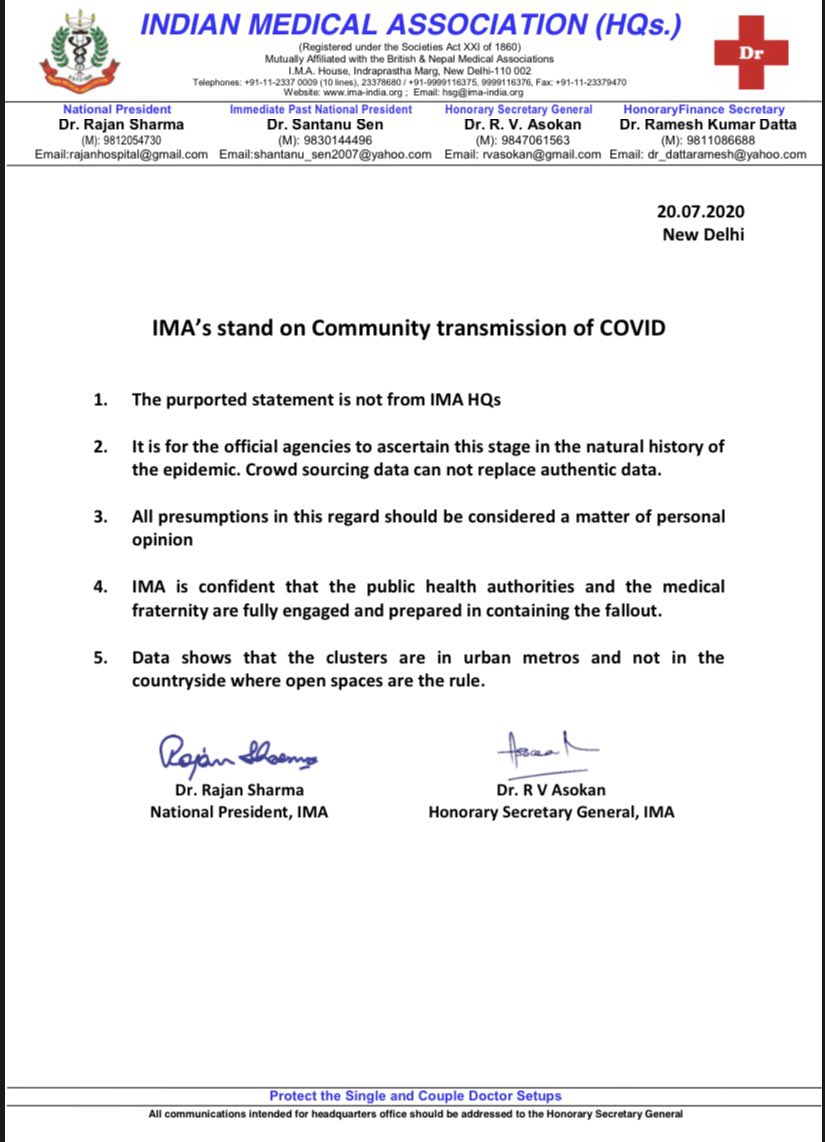
Any other leader or organisation that had admitted or hinted at community transmission had, later on, changed or retracted their statement. On the heels of Kerala’s admission, the Indian Medical Association too said it was time for the government to acknowledge community spread, a stand it has since distanced itself from.
{kind=link}
{kind=link}
On the evening of June 26, Goa Chief Minister Pramod Sawant conceded that community transmission had begun. “We will have to say there is community transmission, we have to accept it,” he was quoted in a tweet by the news agency, ANI. However, a week later, he retracted the statement.
“For some reason admission of community transmission makes policy makers uncomfortable,” said Anant Bhan, a doctor and researcher in global health, bioethics and health policy.
“In the early days [containment stage] you could pretend that you could get rid of it [the virus] and keep doing the same thing... isolate, quarantine; isolate, quarantine,” said Muliyil. “Then you suddenly realise, ‘Oh no! It [the virus] is everywhere.’ So, at least then you call it community transmission.”
Admission of community transmission cannot be seen as a political failure, Muliyil stressed. “You are fighting the virus... it is just that the virus is smarter than us.”
How to tackle community transmission
“Once you have got the virus all over [community transmission phase], catching a few people and putting them in quarantine is counterproductive,” said Muliyil. “It doesn’t work like that.”
Furthermore, India does not need to abandon contact tracing as there would be still some utility for it, especially in areas where the number of cases are growing, said Bhan. “The real question to ask is: What are we doing knowing what we do about the pandemic?”
What works in tackling community transmission is encouraging people to wear masks, wash hands regularly and maintain social distance--behavioural changes that need to be community-driven and monitored, as IndiaSpend reported on July 7. A localised approach depending on the needs and resources of the community works best once community transmission has set in, according to the Centers for Disease Control and Prevention (CDC), which confirmed possible community spread in the US in February.
Following confirmation of community transmission, Kerala, heeding scientific advice, opted to lock down specific clusters to contain the spread, said the state’s health minister K.K. Shailaja to ANI.
Meanwhile, cities such as Delhi, Mumbai and Chennai, which have thousands of active cases, continue to utilise large amounts of resources to quarantine people in hospitals and COVID care centres. In the process those needing urgent hospital care are falling through the cracks, as IndiaSpend reported in June.
By September 1, India might have as many as 3.5 million COVID-19 cases, the Indian Institute of Science has predicted. As cases increase rapidly, isolation and quarantine would have limited effectiveness, suggested experts.
By sending out a stronger and clearer message that only severe COVID-19 cases need hospitalisation while mild and asymptomatic cases should isolate at home, the country would be able to utilise its limited healthcare resources more effectively, said Muliyil. This would result in better care, improved trust and reduction in stigma.
With a vaccine unlikely to be available till at least 2021, Muliyil was also in support of herd immunity. Dharavi in Mumbai had fewer new cases now because the community had, potentially, developed herd immunity already, he reasoned. India’s only option was a community-driven approach that included social distancing but not a lockdown, felt Muliyil.
Fight stigma with transparency
Transparency and regular communication are key to building trust between the government and the public. “The ethical requirement is that you have transparency, that you have open sharing of information, that you build trust with the public,” Bhan said. “This would promote more compliance with government messages and community leaders could be involved.”
However, the government has discontinued regular press briefings. After its June 11 briefing, the next one was held about a month later on July 9. This lack of transparency is hurting India, added Bhan.
The ICMR conducted a sero-survey in April. Researchers visited 28,595 households across 83 districts, and drew blood from 26,400 individuals to test for antibodies against COVID-19. Based on that survey, ICMR in June ruled out community transmission. However, the details of the survey have not been made public yet.
This is not the first time the Indian government has been opaque on an issue relating to public health. In May 2017 when there were three confirmed cases of Zika from Gujarat, the health journalists in India were informed by a WHO news bulletin. The government was not forthcoming with information.
Another big challenge that India faces is the stigma associated with COVID-19. “People who fall sick should not fear that their family members might be quarantined, and, hence, refuse to seek care,” said Muliyil. By the government’s own admission the stigma has caused “hostility” and “chaos”.
It is also important the government decides on the terminology quickly and chooses what is best and easy for people to understand, said Angela Rasmussen, a virologist at Columbia University, while answering a question from IndiaSpend during an ICFJ webinar. “Causing confusion would only get in the way of handling the pandemic,” she said.
This lack of adequate communication is also affecting healthcare seeking behaviour, according to experts. “The [current] system is preventing people from seeking early healthcare,” said Muliyil.
How to tackle community transmission:
- Renewed focus on washing hands, hygiene and social distancing
- Masks recommended in public
- Community-driven and monitored behavioural changes
- Hospitalisation recommended only for those with severe symptoms
- Home isolation for the asymptomatic and mild cases
Source: WHO, Health experts
(Shetty is a reporting fellow with IndiaSpend)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
