Road Accidents Killed 17 Indians Every Hour, Even As Trauma Care Remains Ill-Equipped

Mumbai: “Brake laga” was the last thing Faizan Mithaiwala, then a class XI student, remembers telling his friend as they crashed on the old Pune-Goa highway on a rainy day in June 2011. He was riding pillion, as they made their way to Lonavala, a hill town 85 km south-east of the state capital Mumbai, for the weekend.
The details of the actual crash are still a blur for Mithaiwala. A tempo traveller doubled up as an ambulance and he was rushed to a local hospital near Khopoli, 70 km south-east of Mumbai. But, he had to be moved to another hospital in Panvel, 37 km on the way back to Mumbai, as the one in Khopoli did not have the facilities to treat him. His friend had a fracture on his right hand.
Mithaiwala had massive facial trauma, blood loss, and a brain injury. His right eye was damaged. Two days later, he was shifted to Mumbai’s Saifee Hospital. Ten months in and out of hospitals, expenses of more than Rs 5 lakh, and a major facial reconstruction surgery later, Mithaiwala survived.
He is among the more fortunate victims of road accidents, which kill 17 people every hour in India, on average, according to the latest data from the Ministry of Road Transport and Highways.
Yet, none of the 80 hospitals and medical colleges supported to be upgraded to trauma-care centres during 2012-2017 were functional as of August 2019, government data show. Courses such as advanced trauma life support (ATLS) are not mandatory for doctors in India, experts said, while emergency care centres are spread out unevenly, often manned by junior doctors, and the few that are well-equipped are overburdened, leaving trauma care unprepared.
53 road accidents, 17 accident-related deaths every hour
Nationwide, 467,044 road accidents were reported in 2018--or 53 every hour, on average--an increase of 0.46% compared to 2017, according to the Road Accidents in India 2018 report released in September 2019. These crashes killed 151,417 people--or 17 every hour, on average--2.4% higher than in 2017, and injured 469,418 people.
A third of the road-accident deaths reported were in urban areas, which accounted for 41% of all reported accidents, while two-thirds were in rural areas, data show.
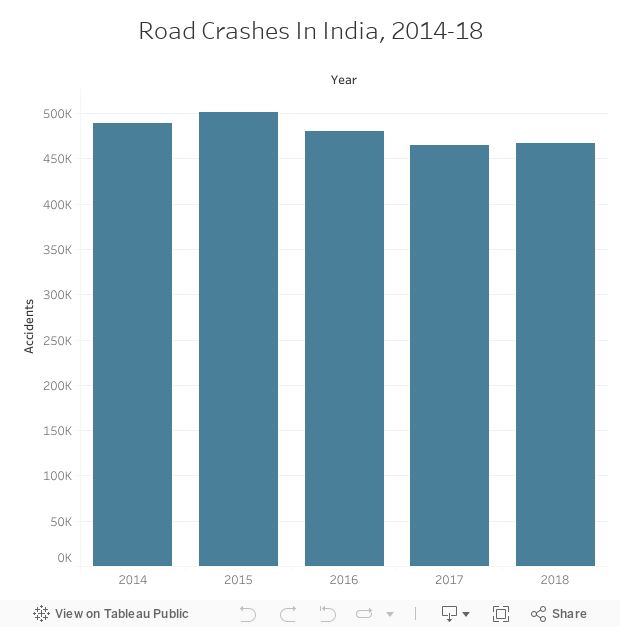
Source: Ministry of Road Transport And Highways 2018
The report classifies accidents into four categories: fatal, grievous injury (requiring hospitalisation), minor injury and non-injury.
Minor-injury accidents accounted for the largest share (36%), followed by fatal accidents (30%) and grievous-injury accidents (27%). The rest (7%) were non-injury.
Grievous-injury accidents “underline the need for provision of Good Samaritan laws and provision of free healthcare during the golden hour to save lives”, which has now been made part of the Motor Vehicles Amendment Act 2019, the report said.
National Highways, which constitute 1.94% of India’s road network, accounted for 30.2% of road accidents and 35.7% of deaths reported in 2018. State highways, which account for 2.97% of the country’s road length, accounted for 25.2% and 26.8% of accidents and deaths reported, respectively.
Between 2014 and 2018, road accidents reported in rural areas rose by about 5%, while deaths and injuries as a result of these accidents rose 20.5% and 2.3%, respectively.
India, which has the second-highest population globally, reported the most road-accident deaths among 199 countries, according to the World Road Statistics 2018 report from the International Road Federation, a not-for-profit based in Geneva, Switzerland, which works on the transport sector. However, India’s incidence of 11 road-accident deaths per 100,000 population ranked fourth globally, and is lower than Iran (20), the Russian Federation (14) and the USA (12).
Reducing road-accident deaths and injuries by 50% and sustaining it over a period of 24 years could generate an additional flow of income equivalent to 14% of India’s 2014 gross domestic product (Rs 125 lakh crore or $2.03 trillion), a January 2018 study by the World Bank said.
Access to emergency care saves lives
The ‘golden hour’ is the first hour after trauma. If proper and timely first aid is given during that time, road accident victims have a higher chance of survival, according to the ‘The Golden Hour’ handbook.
Of 45 million deaths in low- and middle-income countries every year, 54% are due to conditions “potentially addressable by pre-hospital and emergency care,'' according to this 2015 study from the World Health Organization (WHO).
The ministry’s report on road accidents cites the case of Tamil Nadu in this context. Between 2017 and 2018, the state saw a 24% decline in road-accident deaths, data show. This decline is attributable to “multi-pronged initiatives” such as better road-traffic enforcement and an improvement in emergency care, the report said.
Emergency care has been improved with 78 trauma-care centres being set up in the state, the report added. The emergency response time fell with the deployment of 936 ambulances and 41 first-responder bikes. The state also introduced a mobile application that captures location details so that emergency help can reach the accident spot faster.
“Ideally, the hospital needs to be equipped with emergency care--trained doctors and nurses--available 24x7, as well as all equipment that is needed,” said Nitin Jagasia, head of Emergency Medicine at Apollo Hospital, Navi Mumbai. The emergency team needs to be trained in trauma care so that they can start emergency care immediately rather than waiting for a specialist.
In addition to physical injuries, patients also face psychological issues, Jagasia added. “Rehabilitation in India is very scarce, there are very few hospitals or care providers in this field.”
Trauma care in India’s public healthcare
The Centre launched a pilot project for “Strengthening Emergency Facilities along the Highways” in the year 2000, which has since been modified as a scheme titled “Assistance for Capacity Building for Developing Trauma Care Facilities in Government Hospitals on National Highways”.
The objective was to bring down preventable deaths due to road accidents to 10% by developing a pan-India trauma-care network in which no trauma victim has to be transported for more than 50 km. A designated trauma centre was to be made available at every 100 km.
Under this scheme, 116 district hospitals and medical colleges in 17 states were identified to be supported during the 11th five-year plan (2007-2012). Of these, 105 were found to be functional--58 were Level III trauma-care centres, 57 were Level II and one was Level I--according to a Ministry of Health & Family Welfare brief released in August 2019.
The Ministry of Health & Family Welfare categorises trauma care as follows, based on the WHO guidelines:
Level IV: Provided by appropriately equipped and manned mobile hospitals or ambulances.
Level III: Provides initial evaluation and stabilisation (surgically, if needed). Comprehensive medical and surgical in-patient services provided to those patients who can be maintained in a stable or improving condition without specialised care. Emergency doctors and nurses available round-the-clock. Physicians, surgeons, an orthopaedic surgeon and an anaesthetist available round-the-clock to assess, resuscitate, stabilise and initiate transfer as necessary to a higher-level trauma-care service. Should be located at a distance of 100-150 km from each other.
Level II: Provides definitive care for severe trauma patients. In-house emergency physicians, surgeons, orthopedicians and anaesthetists available to trauma patients immediately on arrival. On-call facility for neurosurgeons and paediatricians. Should be located at a distance of 300-450 km from each other.
Level I: Provides the highest level of definitive and comprehensive care for patients with complex injuries. In-house emergency physicians, nurses and surgeons available to trauma patient immediately on arrival. Services of all major super specialties associated with trauma care available 24x7. This should be located at a distance of 600-700 km from each other.
During the 12th plan (2012-17), 85 trauma-care facilities were identified for support, and 80 have been supported. However, none of them are functional, the brief noted.
As a result, existing trauma-care centres are disproportionately burdened.
For instance, about 90% of the cases that Advanced Trauma Centre at the Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, receives are from nearby areas (up to 200 km), though cases also come from Jammu & Kashmir, Sameer Aggarwal, professor and nodal officer at the Advanced Trauma Centre said. The 100-bed centre, which caters to nearly 30 million people, has an occupancy rate of 200%, Aggarwal added. “At any given time, we have about 100-150 patients on [a] trolley because we are the only Level I trauma centre in this region.”
Level III trauma-care centres (TCC) in Maharashtra--which reported the second-highest road-accident deaths in 2018--are spread out unevenly, according to a 2017 Comptroller and Auditor General report. Level III TCCs should be at a distance of 100-150 km from each other, according to the guidelines from the Ministry of Health & Family Welfare. Of 69 Level III TCCs in the state, 38 were at a distance of 50 km from each other and 14 at a distance of 50-100 km, covering mainly the western and central parts of the state, the audit found. “The remaining 17 TCCs registered their sporadic presence in the eastern, southern and northern parts of Maharashtra,” the report added.
Further, of 18 Level III TCCs audited, 13 were non-functional or partially functional as of January 2017 due to inadequate manpower, shortage of equipment, and incomplete infrastructure such as electric works, compound walls and water supply. Only 136 of the 270 posts in the 18 audited TCCs were filled, the audit found.
A 14-bedded trauma-care centre in Gujarat’s Patan district, established at a cost of Rs 1.59 crore--enough to pay for trauma care expenses for a month for nearly 900 patients, on average--could not be put to use due to non-appointment of medical and paramedical staff, according to another CAG report from 2018. As of August 2017, one post each of orthopaedic surgeon and anaesthetist, three posts of a medical officer, and six posts of 24-hour paramedics were vacant, the audit found.
Emergency care unprepared: experts
Courses such as Advanced Trauma Life Support (ATLS) are not compulsory for doctors and nurses in India, Mahesh Chandra Misra, former director of the All India Institute of Medical Sciences, New Delhi, told IndiaSpend. In the US, implementation of ATLS courses has made sure 24-hour injury mortality is down to 4% while in India it remains at 10%, he added.
Emergency centres are staffed with junior doctors in both private and government hospitals, which may put the life of the patient at risk, Misra said. Further, there are delays in patients’ reaching trauma-care centres.
Only 15% of accident victims are brought to trauma-care centres by an ambulance while the rest are taken to nearby health facilities by relatives or bystanders, Misra added. “The health facilities are small and cannot deal with a major injury. It sometimes takes them more than 48 hours to determine the injury.”
Trauma impacts the poor and low-income groups--as most injuries and deaths are among two-wheelers and pedestrians--Misra said, and trauma-care centres need high investment, explaining why trauma care has not taken policy centre-stage. Most of these patients are taken to government hospitals since private care is unaffordable and patients often do not have insurance cover, he added.
Private medical hospitals--which have all the facilities required for trauma care such as CT scans, operation theatres and qualified doctors--run at very low occupancy rates, Misra said. “There is a mismatch here, oversupply of patients to the government sector and undersupply in the private sector.”
The government has many schemes such as Ayushman Bharat to cover the costs, he said, adding that if this can be utilised--if the government can buy these services from the private sector--lives will be saved.
“Accidents usually happen on stretches of highways that are not populated, or far away from health facilities, or in mountains and other hard-to-reach places,” Patanjali Dev Nayar, regional advisor for the WHO, said. “So getting there is always a challenge.”
“Trauma care such as polytrauma care can be integrated into primary health,” Nayar added. “For example, a blood bank that can help an accident victim can also help a mother who is bleeding in postpartum pregnancy. That is why we [WHO] advocate integrating polytrauma care within the primary healthcare facilities over building separate trauma centres.”
“Health is a concurrent subject--there are too many agencies involved in the implementation,” he added. “So sometimes the Centre starts something but the state may not take it forward. Additionally, there is not a lot of advocacy around issues such as trauma care and not a lot of money is dedicated to it.”
(Salve is an IndiaSpend contributor. This article is part of the Road Safety Media Fellowship 2019.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
