With Health Funds Unused, 24%-38% Shortfall In Medical Staff Across India

Mumbai: There is a 24%-38% shortfall in the availability of medical personnel at primary health centres, sub centres, and community health centres in 28 states/union territories of India, according to the latest audit by the Comptroller and Auditor General (CAG) of India.
In the first part of this series on the CAG’s assessment of the National Health Mission (NHM), we looked at issues of financial management. In this concluding part, we detail the lack of physical infrastructure and human resources at public health facilities.
The survey found that 73% of sub centres were more than 3 km from the remotest village, 28% were not accessible by public transport and 17% were unhygienic. In 24 states, instances of non-availability of essential drugs were observed. In eight of these states, essential medicines/ consumables such as vitamin-A, contraceptive pills, oral rehydration solution (ORS) packets and essential obstetric kits were not available at select health facilities.
NHM, launched in 2005, is India’s largest health programme aimed at providing universal access to healthcare. It passes on funds to state health societies to strengthen local health systems, institutions and capabilities. But, as we reported in the first part of the series, states are not utilising these funds optimally and there has been a 29% rise in the balance left with states in the five years leading to 2016. The results of this are visible in the infrastructure and human resource gaps across health facilities in India.
77%-87% community health centres don’t have specialists
NHM aims at ensuring uninterrupted and quality healthcare by increasing the availability of doctors, specialists, paramedical staff, auxiliary nursing midwives (ANMs) and accredited social health associates (ASHAs). State governments are supposed to fill up existing vacancies with new contractual appointments for which the Centre provides funds.
However, CAG noted in its report, shortfalls in the availability of staff at health centres was more than 50% in five states--Bihar, Jharkhand, Sikkim, Uttarakhand and West Bengal. Bihar had the most shortages in community health centres (92%).
Across the states surveyed, it was found that 77% to 87% community health centres were functioning without specialist doctors such as obstetricians/gynaecologists and paediatricians. The ministry’s response was that the shortage was due to inadequate availability of personnel and even irrational deployment of doctors and specialists by state governments.
Source: Comptroller and Auditor report
In 13 states--Andhra Pradesh, Arunachal Pradesh, Assam, Chhattisgarh, Haryana, Himachal Pradesh, Karnataka, Madhya Pradesh, Odisha, Punjab, Rajasthan, Uttar Pradesh and Uttarakhand--67 of 305 primary health centres surveyed (22%) were functioning without any doctor.
In 13 states, ANM/health worker (female) was not posted in 10% of sub centres. Male health workers were not posted in 65% of 22 states. Female health workers are the primary drivers of maternal health initiatives, but male health workers could complement their services significantly, IndiaSpend reported on March 22, 2017.
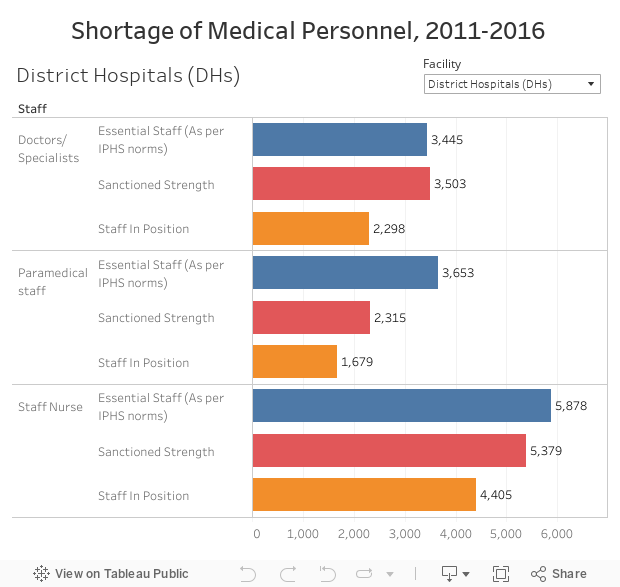
In selected 236 community health centres in 24 states/union territories, only 1,303 nurses were posted against the required 2,360.
Manpower shortage led to unused infrastructure
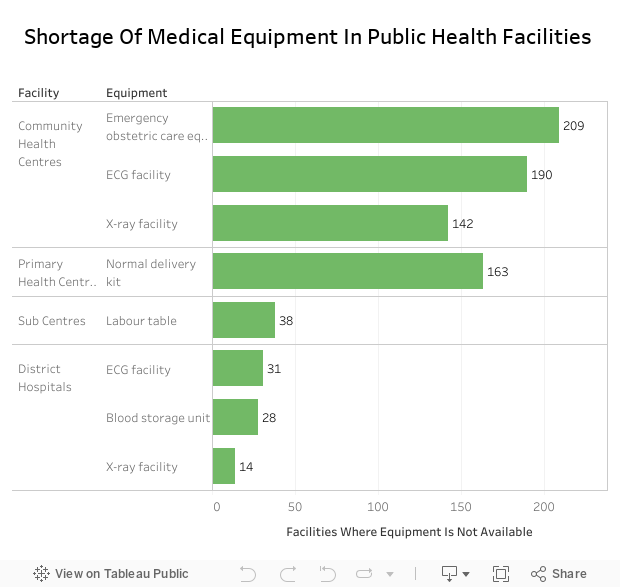
In 20 states, 1,285 works, though completed, were not commissioned or made functional. In 17 states, 428 equipment for ultrasound, X-ray, ECG , cardiac monitoring, incineration, operation theatres and blood storage costing Rs 30 crore were lying idle/unutilised due to non availability of doctors and trained manpower.
The ministry attributed the shortfall of health facilities largely to shortage of funds in the 12th Five Year Plan: Against the requirement of Rs 1,93,405 crore, only Rs 91,022 crore was made available. However, the CAG did not accept this response because there were substantial unspent funds with the states.
Audit showed that health centres are not clean, have no electricity, water, are poorly connected
Financial support is provided to states under National Rural Health Mission (NRHM) to strengthen the health system including the supply of drugs. States are being incentivised up to 5% of their total outlay under NRHM to prepare policy and establish systems for the free distribution of essential drugs, robust procurement system, and so on.
The survey of 1,443 sub centres, 514 primary health centres, 300 community health centres and 134 district hospitals by the CAG revealed that states are fulfilling their NHM mandate. Some health facilities were functioning in unhygienic environment and/or were inaccessible by public transport. Other infrastructural issues included poor condition of the buildings, non-availability of electricity and water supply, non-availability of separate wards for male and female beneficiaries, non-functional labour rooms and so on.
| Health Facilities, By State, 2011-2016 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sub Centres | Primary Health Centres | Community Health Centres | District Hospitals | |||||||||
| Factors found deficient | No. | % | States /UT | No. | % | States /UT | No. | % | States /UT | No. | % | States /UT |
| Distance of more than 3 km | 1031 | 73 | 29 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Not accessible by public transport | 404 | 28 | 28 | 104 | 20 | 24 | NA | NA | NA | NA | NA | NA |
| Unhygienic surroundings | 236 | 17 | 27 | 96 | 19 | 27 | 78 | 26 | 19 | 40 | 30 | 24 |
Source: Comptroller and Auditor report
Mobile medical units were not operational in Chhattisgarh, Himachal Pradesh, Mizoram and Uttar Pradesh while these were partially operational in 10 states.
Shortfall in the construction of sub centres, primary health centres in 25 states and community health centres in 17 states ranged between 32% to 44%. In four states (Kerala, Manipur, Mizoram and Uttar Pradesh), 400 works costing Rs 2,208 crore were awarded on nomination basis.
Source: Comptroller and Auditor report
In eight states, of the Rs 175 crore allotted to buy ambulances, Rs 156 crore (89%) remained unutilised. Some of the irregularities observed by the audit were administrative delays, tendering process for procurement process not being initiated, diversion of funds for other purposes and so on.
Medical kits with ASHA workers not replenished
In 24 states, the CAG reported instances of non-availability of essential drugs. In eight of these, essential medicines/ consumables such as vitamin-A, contraceptive pills, oral rehydration sachets, drugs to deal with reproductive tract infection and sexually transmitted infection, essential obstetric kits and so on were not available in selected health facilities.
Free supply of essential drugs at public health facilities has been made mandatory in India since 2014. But a study by the State Health Resource Centre at Raipur, reported by IndiaSpend on June 13, 2018, showed that only 58% of prescribed medicines were available at primary health facilities in Chhattisgarh. This forced patients to buy drugs, at higher prices, from private pharmacies.
Every ASHA is to be provided with a drug kit containing a set of drugs, equipment and product. These kits are critical because they enable health workers to provide basic care to the community.
| ASHAs Not In Possession Of Item/Medicine | ||
|---|---|---|
| Item | Number surveyed | Percent of total ASHAs |
| Disposable delivery kit | 3,249 | 83 |
| Blood pressure monitor | 3,170 | 81 |
| Thermometer | 1,060 | 27 |
| Pregnancy kit | 1,428 | 28 |
| Weighing scale (for newborns) | 887 | 23 |
| Deworming pills | 1,299 | 33 |
| Paracetamol tablets | 1,006 | 26 |
| Iron pills | 878 | 22 |
Source: Comptroller and Auditor report
Items such as disposable delivery kit, blood pressure monitor, thermometer, pregnancy kit, weighing scale and medicines like deworming pills, paracetamol tablets and iron pills are essential for providing basic reproductive and child health services by the ASHA network. In 10 states (Bihar, Chhattisgarh, Himachal Pradesh, Kerala, Madhya Pradesh, Maharashtra, Meghalaya, Rajasthan, Sikkim and West Bengal), delays in replenishment of drug kits, and non-availability of ASHA kits were noticed.
Shortfalls in administration of iron folic acid tablets were noticed in all 28 states. Similarly, in four states (Arunachal Pradesh, Jammu and Kashmir, Manipur and Meghalaya), less than 50% of pregnant women were immunised with both doses of the tetanus toxoid vaccine (TT1 and TT2).
The ministry has stated that it is now promoting the use of IT software at public health facilities to control the stock and supply of drugs.
The audit also found that the institutional framework for implementation of the National Quality Assurance Programme was either not in place or was not effective in assuring quality of services across all levels--national, state, district. The programme was launched in 2013 to improve the quality of care in district hospitals, community and primary health centres across the country.
Of 716 facilities in 19 states, an internal quality assurance team was constituted in only 308 facilities (43%). In 541 health facilities of 15 states, the system of periodic internal assessment was formulated only in 114 (21%) facilities.
Series concluded. You can read the first part here.
(Salve is an analyst with IndiaSpend.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
